 企業(yè)郵箱
企業(yè)郵箱






Study on the Bacterial Count of Viable Tissue of Burn Wound
作者:Rong Xiang Xu 出版社:KARGER 發(fā)行日期:In 2004INTRODUCTION
In order to verify the ability of BRT with MEBT/MEBO to inhibit localized infections, we conducted a study on the bacterial number of viable tissue of burns wounds. The results showed that MEBO therapy effectively controlled bacterial number to less than 104 per gram of viable tissue during the whole treatment procedure. This result suggests a strong capacity for the prevention of wound invasive infection.
MATERIALS AND METHODS
The backs of 28 adult healthy guinea pigs of either sex were depilated and scalded on both sides by a hot test tube to obtain full-thickness necrotic wounds with a diameter of 3 cm. One wound on each side of every animal randomly served as a blank exposed group (control group) while the other side served as the BRT with MEBT/MEBO treatment group (test group). Wounds in the control group were kept clean and allowed to heal spontaneously, while wounds in the test group received BRT in the typical manner. Twenty-eight animals were harvested seven at a time at four different time intervals (days 3, 6, 10, 20 post injury). Viable tissue underlying the wounds were sampled for bacterial count and compared with normal subcutaneous tissue.
Viable tissue sampling and bacterial counting
The wound surface was sterilized with iodine and alcohol after each animal was sacrificed. Sterilized tissue scissors were used to cut tissues from each wound without touching the deep fascia and muscle tissue. The sampled wound tissues were spread flat in sterilized cloth with the subcutaneous tissue exposed. Sterilized ophthalmic scissors were then used to excise viable subcutaneous tissues (excluding necrotic tissues). The sampled viable tissues were weighed, triturated and diluted. Diluents were inoculated into agar culture medium at a specific concentration and cultured for 48 h (at a constant temperature of 37C). Bacterial colony count was performed from which total bacterial count and bacteria per gram of viable tissue were obtained.
RESULTS
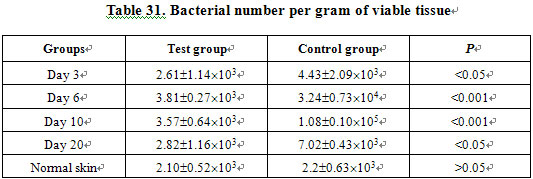
The bacterial number in viable tissues of burns wounds was less than 104/g in both groups, indicating there was no wound invasive infection during the whole test period. However, the bacterial number in wound viable tissue of the test group was significantly less than that in the control group at each observation time (Table 31).
DISCUSSION
There are several general clinical methods for determining wound bacterial determination, including (1) swab culture of wound surface; (2) quantifying bacterial number of full-thickness burns wound; (3) bacterial counting of sub-eschar viable tissues. The first method is easy to perform, but fails to provide appropriate proof for the existence of invasive infection on burns wounds. Clinical application and lack of comparability limit the second method. The third method is usually adopted in clinics to predict the possible success or failure of skin grafting and is regarded as an ideal method for detecting the existence of wound invasive infection. Many authors used this method for early diagnosis of wound sepsis.
In 1983, Bharadulj reported that more than 105 bacteria per gram of sub-eschar viable tissue is diagnostic for wound sepsis. He also found that patients who died from systemic infection bore more than 108 bacteria per gram viable tissue. Other authors agree [Robson VN, et al.]. Therefore, we too adopted this method for the purposes of this study. The results demonstrate that in different stages postburn, no more than 104/g was detected in sub-eschar viable tissues taken from the BRT with MEBT/MEBO group. We also noted that there was no obvious difference throughout all stages although the peak occurred during the period of wound rejection reaction. In the control group, although no infection symptoms were observed on wounds, bacterial number per gram sub-eschar viable tissue increased progressively until a peak of 105/gram during the wound-rejecting reaction period. A significant difference occurred between the two groups. Based upon bacterial number, we see that MEBO had a unique effect in controlling wound infection compared to normal tissue.
There are four dominant sources for burn wound infection: (1) parasitic bacteria in underlying wound viable tissue; (2) burned tissues; (3) external contamination; (4) hematogenous infection. It has been believed for a long while that a dry, clean or sterilized wound environment may lead to a lower incidence of infection than would a damp environment. Some experiments have been conducted while maintaining the wound moist, but the results suggested that a dry wound status was preferable. Therefore, a therapeutic principle of drying the wound was established to prevent infection and dampness was itself regarded as a risk factor for infection. Interestingly, our research reached a contrary conclusion.
A wet environment, according to the general rule, was understood to provide a favorable surrounding for bacterial growth despite the realization that tissue necrosis, which results from a dry wound status, provides a much more nutrient substrate for microbial proliferation. Accordingly, we advocated that a physiological moist environment, assuming appropriately regulated humidity, was favorable for tissue recovery as well as enhancement of endogenous resistance to infection with its resultant reduction of infection. Furthermore, it is well understood that burn wound infections are caused by a variety of factors and that each of these should be accounted for along with a clean wound environment. For example, blocked sub-eschar drainage resulted from dryness of wound and eschar formation would support the bacterial colonization, thereby increasing the possibility of wound infection. If wounds were kept wet without taking other effective measures, infection would be likely. We invented BRT with MEBT/MEBO in order to maintain the wound in a physiologically moist environment, which, while causing no infection, also allowed for dramatically less bacterial number in sub-eschar viable tissue than in wounds treated by dry therapy. Why? According to the designing theory of BRT with MEBT/MEBO, we had the following analysis.
1. Moist environment for wound: In our study, a “moist” instead of “wet” environment was emphasized. The special formulation of MEBO developed on the basis of Chinese traditional philosophy ensured an appropriate “moist” wound environment. Composed of beeswax and non-water edible plant oil, the dosage form of MEBO has a strong affinity to skin and wound tissues. Its unique structure protects burn tissues from direct immersion by exuded endogenous fluid, prevents bacteria in water from contacting tissues and therefore keeps wounds moist, but not macerated. The physical change of the ointment from semisolid to liquid allows a circulation of ointment across the wound, ensuring effective drug concentration and addressing the requirements of tissue repair. Prior to the invention of MEBO, exposure therapy with the application of other topical drugs was considered as the predominant measure to monitor wound condition. To its credit, wound exposure allowed better assessment of the need for drug renewal as well as for timely drainage and manual discharge of exudation.
2. Unobstructed drainage and isolation: BRT with MEBT/MEBO features an automatic drainage system that enables the timely drainage and discharge of exudation and liquefied products from the wound surface. This mechanism of action destroys the bacterial growth environment, interrupts bacterial nutriment supply, reduces bacterial concentration and therefore effectively arrests bacterial proliferation and invasion. The unique dosage form of MEBO effectively isolates the wound from bacterial contamination originating from the surrounding environment by forming a barrier that actually provides the wound with a clean and relatively “sterile” environment.
3. Drug ingredients and other claims: MEBO also claims to increase local blood flow, promote recovery of the microcirculation, and encourage wound healing. These three factors all enhance the ability of local tissue to resist infection.